The first installment addressing the biomechanical needs of patients’ status post trans metatarsal amputation (TMA) reviewed the major biomechanical challenges these patients face and initial treatment approaches utilizing toe fillers and shank additions. This second column addresses treatment options for patients requiring more proximal control and support.
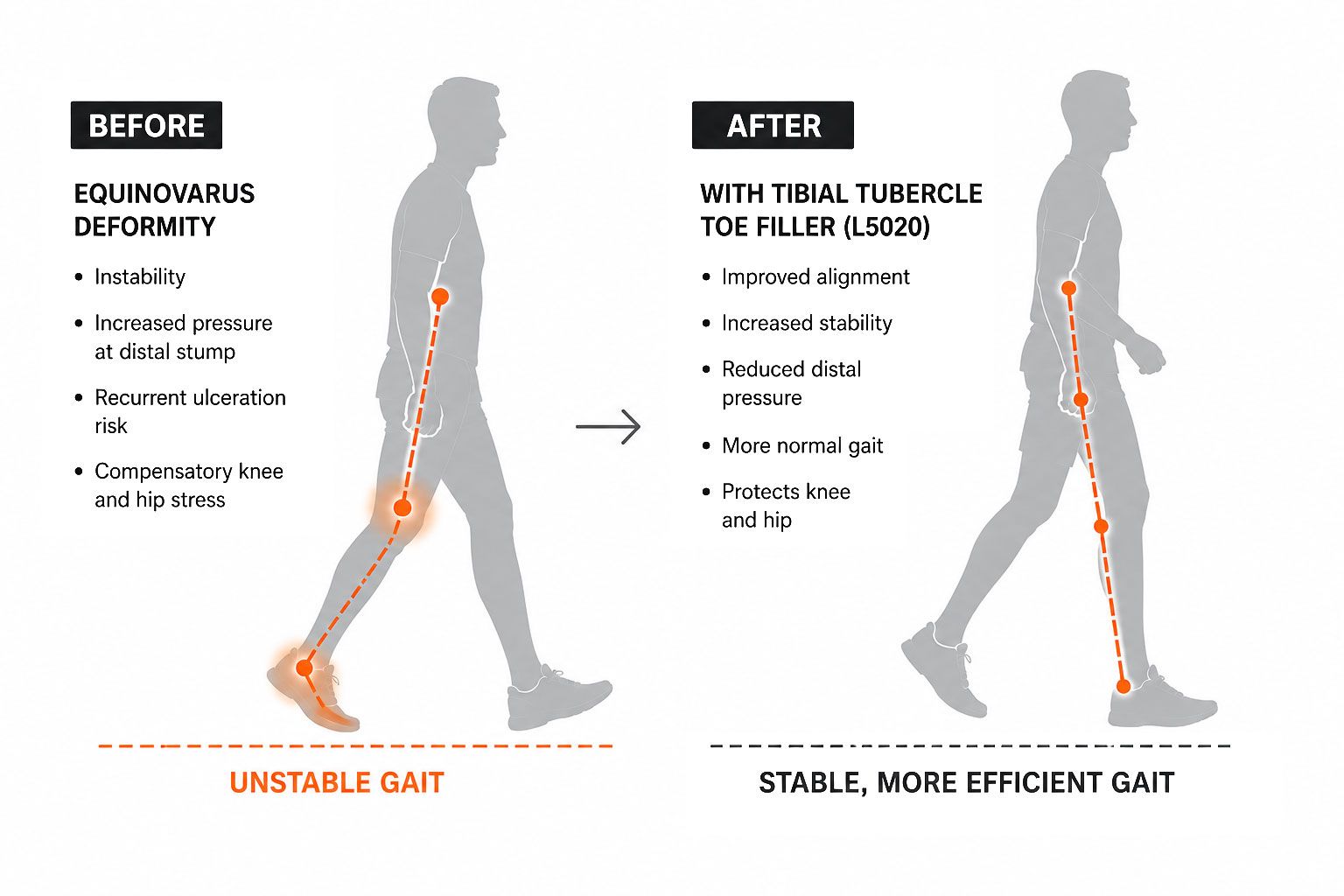
Many patients following a total TMA develop significant equinovarus deformities. For these patients, a simple toe filler (L5000) or a toe filler with rigid carbon reinforcement (L5000 + L2755) is often insufficient to address more advanced biomechanical deficits.
Left unchecked, these patients frequently develop recurrent ulcerations resulting from increased plantar pressures at the distal stump, particularly at the fifth metatarsal base. Others may develop or accelerate knee and hip pathology as these proximal joints attempt to compensate for the equinovarus deformity.
A toe filler with rigid uprights extending well above the ankle joint, can help restore a more normal gait pattern by providing increased mechanical support and preventing shoe buckling. As noted in the prior article, these devices can also store energy and assist forward propulsion during the later stages of gait.
For most adult patients, supramalleolar (SMO) prosthetic devices (L5010) often do not provide sufficient corrective forces because of the limited height and lever arm of the SMO design which extends just superior to the ankle joint. However, a toe filler extending proximally to the tibial tubercle (L5020), with appropriate modifications, can provide adequate corrective forces for many patients with substantial equinovarus deformities and facilitate a more normal gait pattern.
The rigid uprights of a tibial tubercle toe filler function as a lever arm, improving stability and helping maintain the foot in a more neutral position depending upon positioning during casting. These uprights may be fabricated from polypropylene, which is standard, or carbon fiber, which is lighter, provides more efficient energy return, and may be especially advantageous for heavier or more active patients.
Similar to a simple toe filler, the footplate portion of the prosthesis is designed to reduce foot slippage and prevent shoe buckling, thereby reducing pressure at the stump and contributing to a more normal gait pattern.
Many patients following a total TMA develop significant equinovarus deformities. For these patients, a simple toe filler (L5000) or a toe filler with rigid carbon reinforcement (L5000 + L2755) is often insufficient to address more advanced biomechanical deficits.
Left unchecked, these patients frequently develop recurrent ulcerations resulting from increased plantar pressures at the distal stump, particularly at the fifth metatarsal base. Others may develop or accelerate knee and hip pathology as these proximal joints attempt to compensate for the equinovarus deformity.
A toe filler with rigid uprights extending well above the ankle joint, can help restore a more normal gait pattern by providing increased mechanical support and preventing shoe buckling. As noted in the prior article, these devices can also store energy and assist forward propulsion during the later stages of gait.
For most adult patients, supramalleolar (SMO) prosthetic devices (L5010) often do not provide sufficient corrective forces because of the limited height and lever arm of the SMO design which extends just superior to the ankle joint. However, a toe filler extending proximally to the tibial tubercle (L5020), with appropriate modifications, can provide adequate corrective forces for many patients with substantial equinovarus deformities and facilitate a more normal gait pattern.
The rigid uprights of a tibial tubercle toe filler function as a lever arm, improving stability and helping maintain the foot in a more neutral position depending upon positioning during casting. These uprights may be fabricated from polypropylene, which is standard, or carbon fiber, which is lighter, provides more efficient energy return, and may be especially advantageous for heavier or more active patients.
Similar to a simple toe filler, the footplate portion of the prosthesis is designed to reduce foot slippage and prevent shoe buckling, thereby reducing pressure at the stump and contributing to a more normal gait pattern.